
Cardiomyopathy syndrome (CMS) is a severe cardiac disease affecting Atlantic salmon characterized by prolonged periods of usually low-level mortalities.
The disease was first recognized in farmed Atlantic salmon in Norway in 1985 and subsequently in farmed salmon in the Faroe Islands, Scotland and Ireland. CMS is a transmissible disease that has been causally linked to the Piscine Myocarditis Virus (PMCV), closely allied to the Totiviridae.
CMS usually causes mortality in adult or maturing fish after 12 to 18 months in seawater, resulting in substantial economic losses.
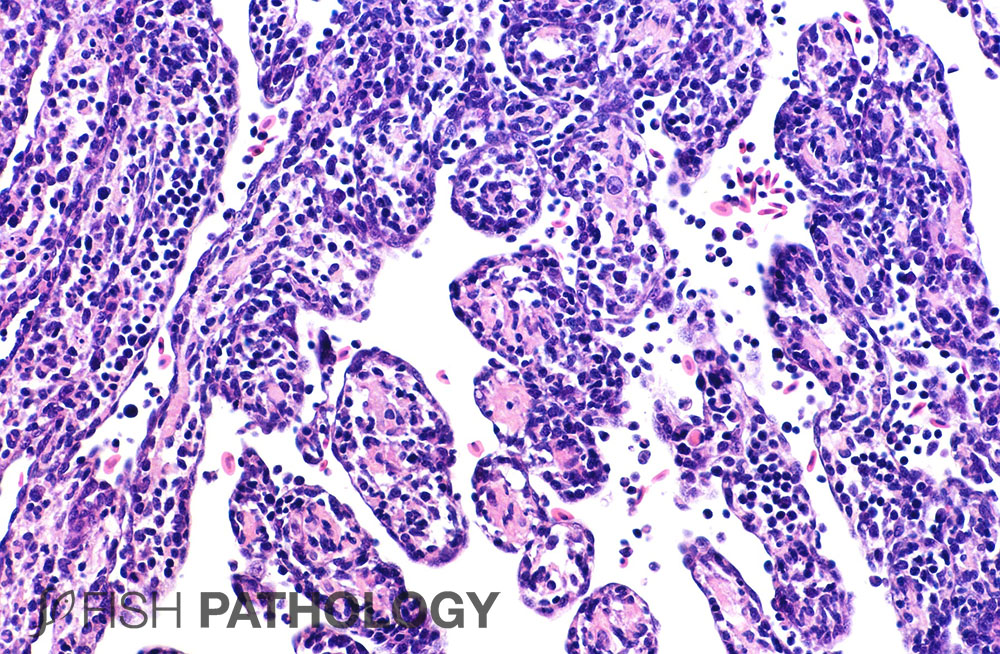
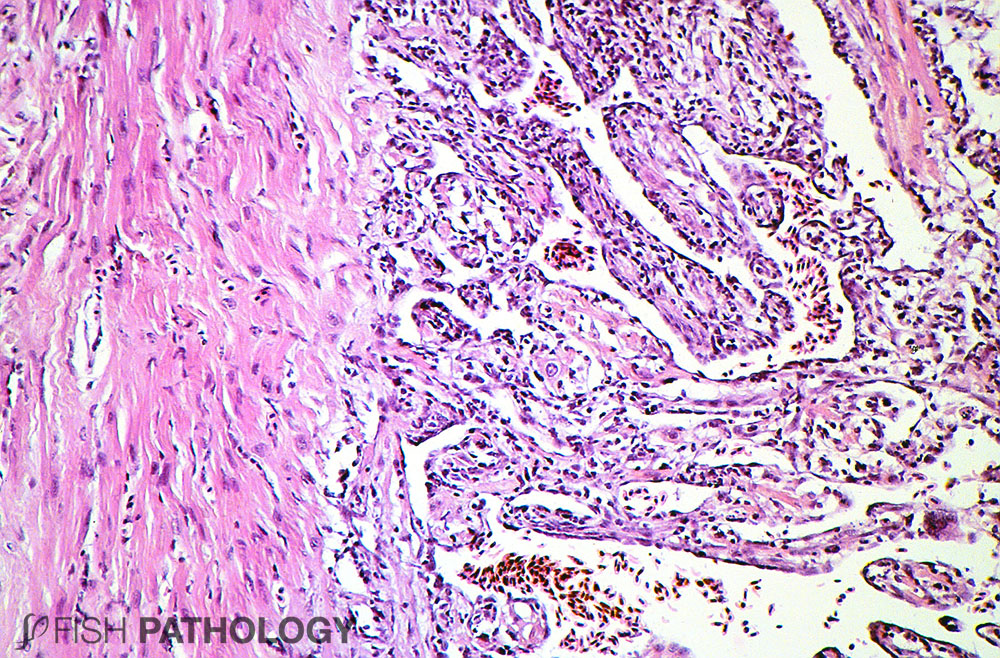
The lesions of CMS start with swollen endocardial cells, an influx of inflammatory cells into the myocardium, accompanied by degeneration, loss of striations and necrosis.
Ongoing phagocytosis of necrotic tissue leads to largely empty myocardial “tubes” filled with inflammatory cells (mostly mononuclear) including macrophages clearing up the debris. In severe cases there is frequently infiltration of lymphocyte-like cells onto the pericardium.

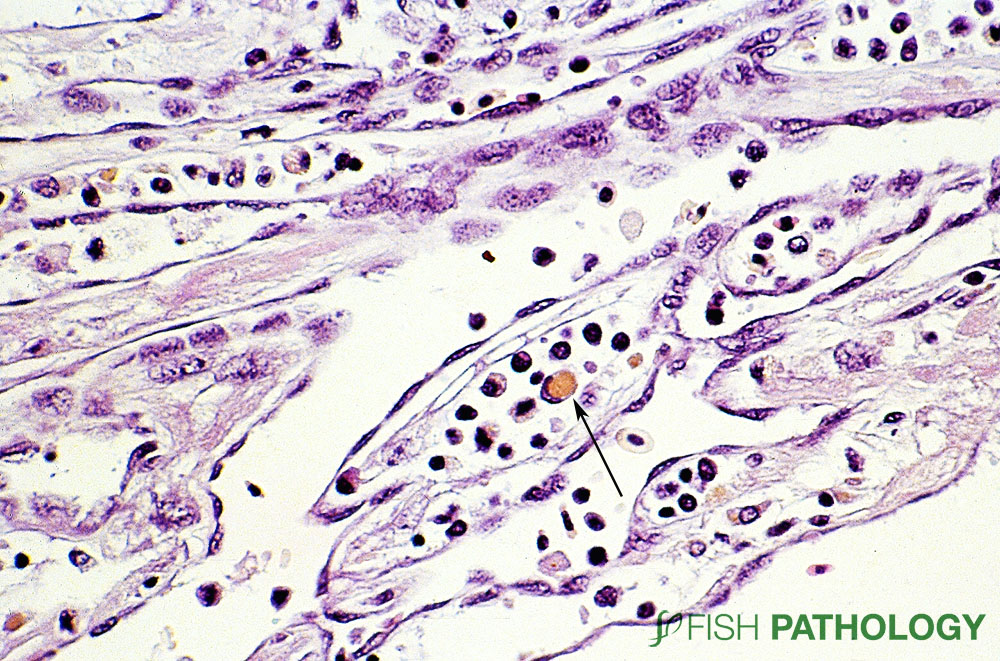
In later stages, ongoing degeneration can often be seen in the face of compensation and regeneration of myocardium.


Such changes include nuclear hypertrophy of myocytes adjacent to severely affected cells. But they can also include clusters of 5-20 myocyte-like nuclei, suggesting the myocardial equivalent of “nuclear rowing” as can be seen in regenerating skeletal muscle.
Liver lesions are typical of “heart failure liver” with zonal degeneration of hepatocytes, a consequence of hypoxia.
REFERENCES
- Ferguson, H.W., T. Poppe, and D.J. Speare. (1990). Cardiomyopathy syndrome in farmed Norwegian salmon Salmo salar L. Dis. Aquat. Orgs. 8:225-231.
- Garseth, Å. H., Fritsvold, C., Svendsen, J. C., Bang Jensen, B., & Mikalsen, A. B. (2018). Cardiomyopathy syndrome in Atlantic salmon Salmo salar L.: a review of the current state of knowledge. Journal of fish diseases, 41(1), 11-26.
- Løvoll, M., Wiik-Nielsen, J., Grove, S., Wiik-Nielsen, C. R., Kristoffersen, A. B., Faller, R., … & Meyerson, M. (2010). A novel totivirus and piscine reovirus (PRV) in Atlantic salmon (Salmo salar) with cardiomyopathy syndrome (CMS). Virology Journal, 7(1), 309.
- Wiik‐Nielsen, C. R., Ski, P. M., Aunsmo, A., & Løvoll, M. (2012). Prevalence of viral RNA from piscine reovirus and piscine myocarditis virus in Atlantic salmon, Salmo salar L., broodfish and progeny. Journal of Fish Diseases, 35(2), 169-171.
