Bacterial kidney disease (BKD) is a chronic systemic infection of salmonid fish, the cause of which is the gram-positive diplobacillus, Renibacterium salmoninarum. Although BKD is most common in salmonids, both farmed and wild, R. salmoninarum is also found in other fish species, such as cyprinids and sablefish Anoplopoma fimbria.
R. salmoninarum grows intracellularly in the phagocytic cells of the fish, resulting therefore in a largely granulomatous host response, although the early response to infection does involve significant numbers of neutrophils.
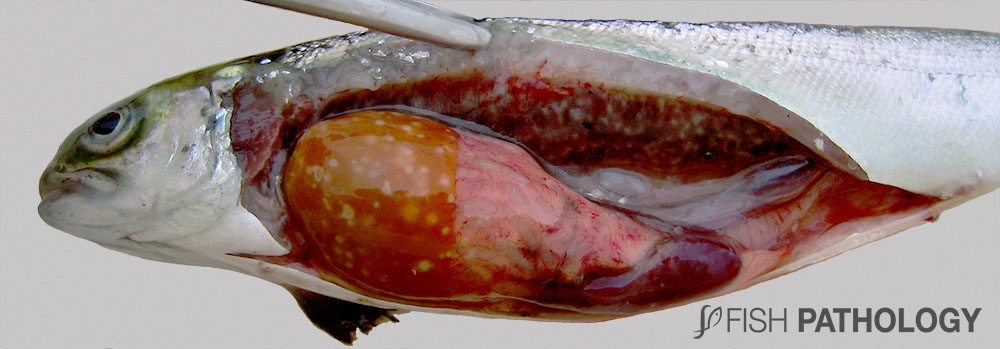
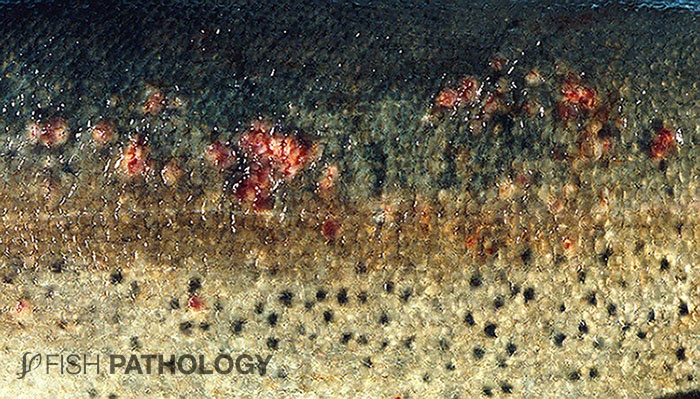
Clinical signs and external lesions are variable and range from darkening and a mottled appearance to the skin, distended abdomen, exophthalmia, petechiae and haemorrhaging around the base of the pectoral fins and the lateral line. Superficial blister with vesicle formation, abscessation and subsequent ulceration may develop in the skin and even cavitations in the musculature can form. Nervous symptoms are encountered if the brain becomes involved; this is not uncommon if the fish are fed long-term antibiotics (those which cannot cross the blood-brain barrier).
Gills and internal organs can be pale, indicating the anaemia that is often present. Given the extent of involvement and destruction of haemopoietic tissue in kidney and spleen, this is probably a myelophthisic anaemia.
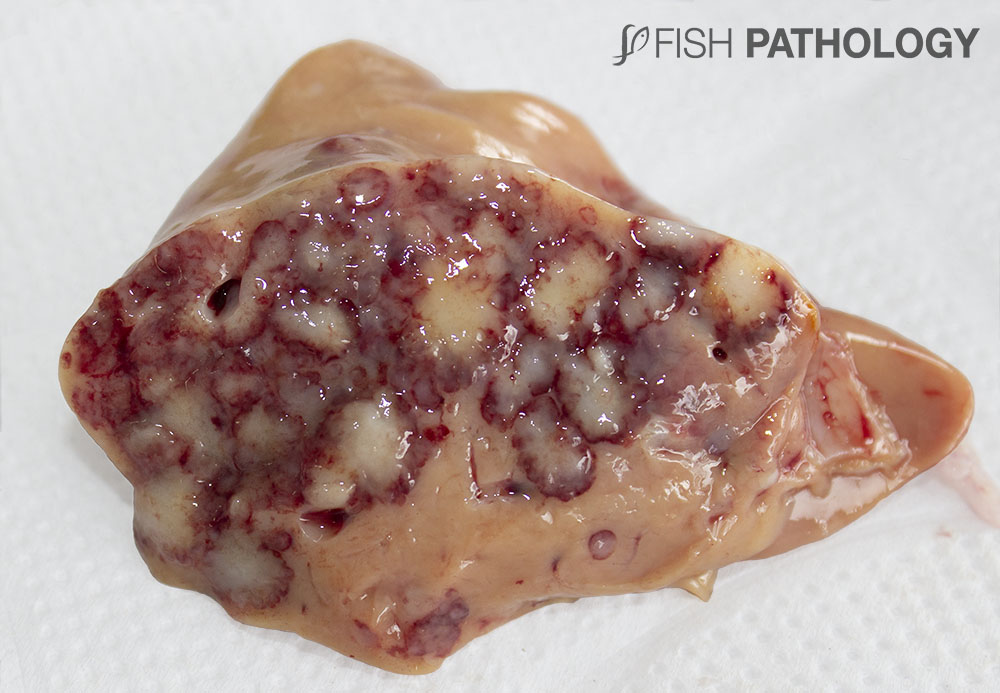
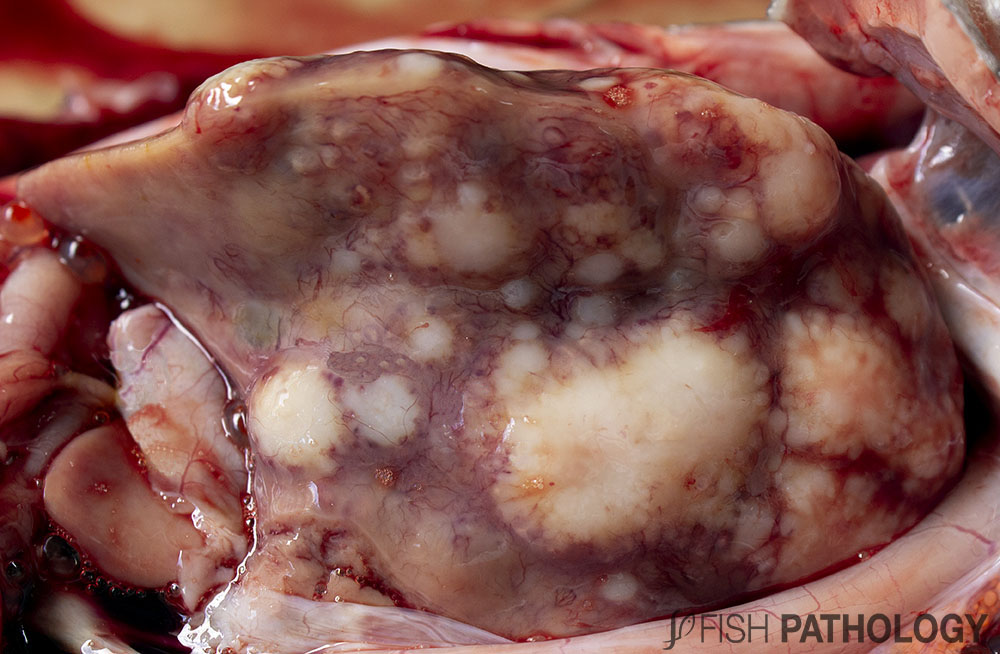
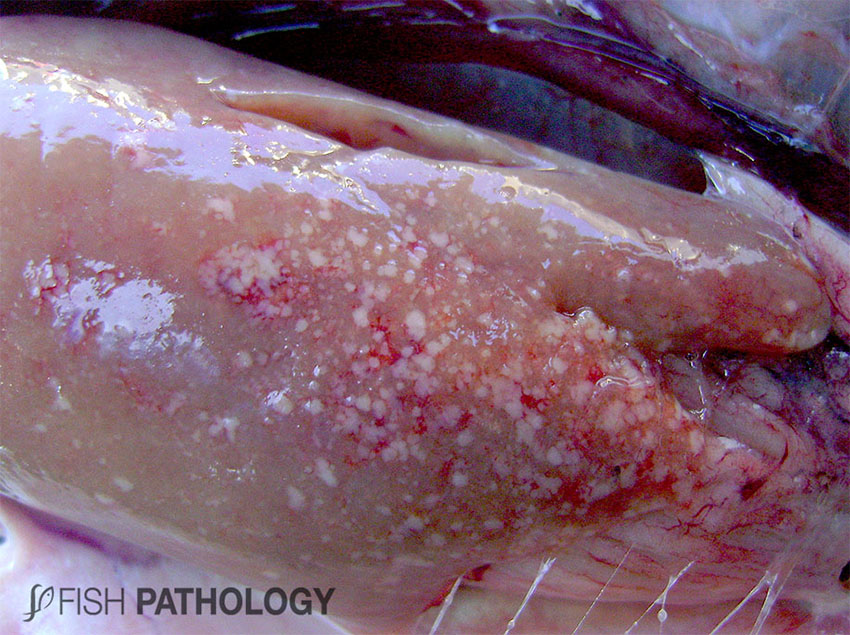
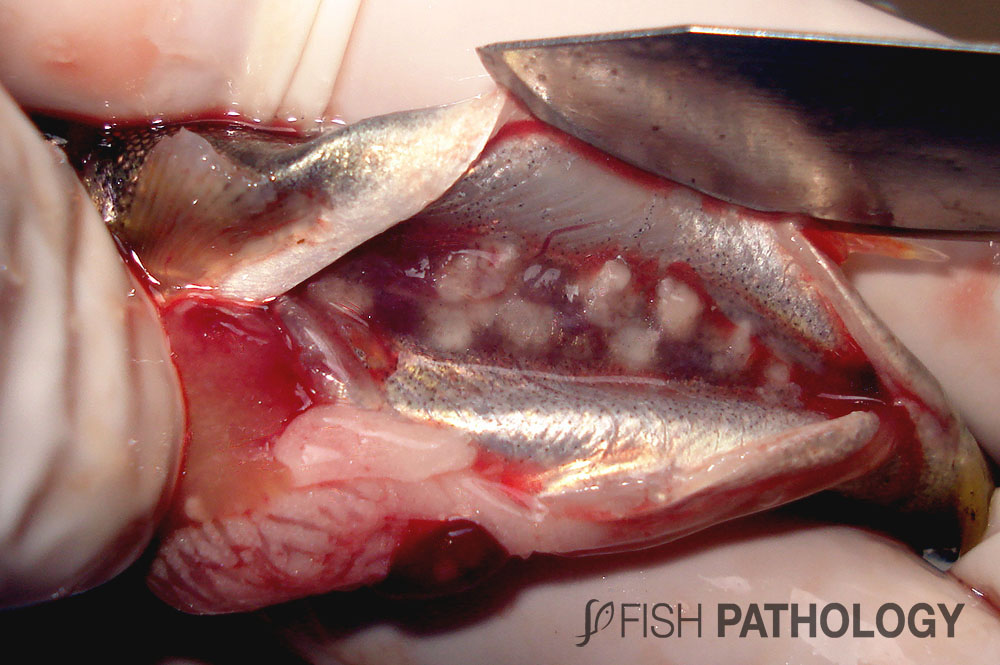
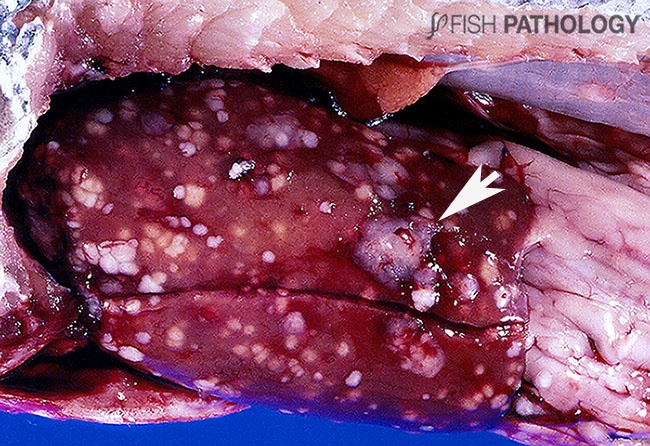
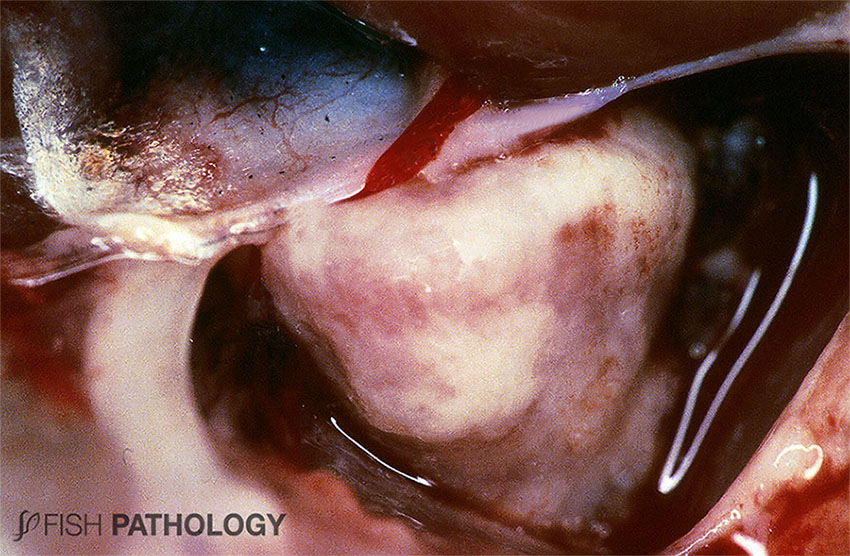
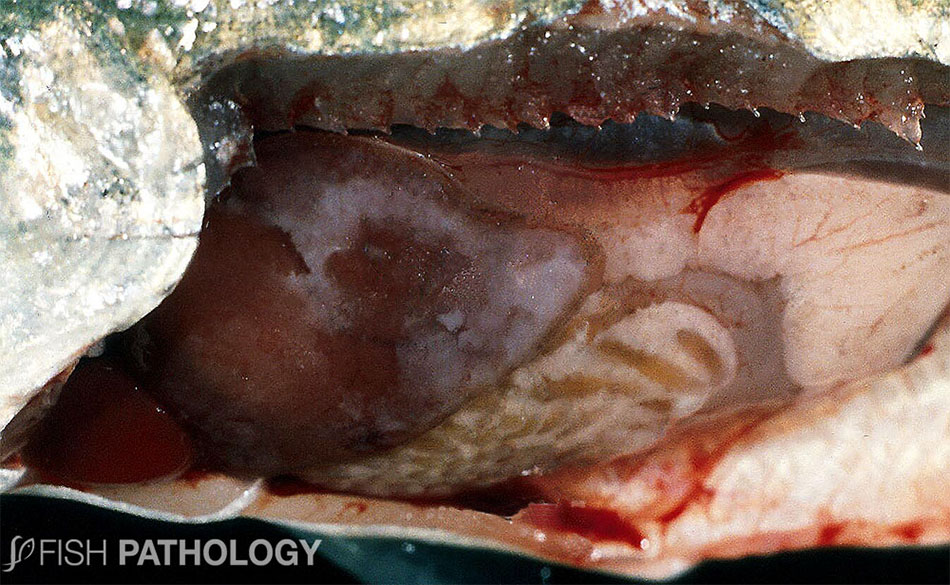
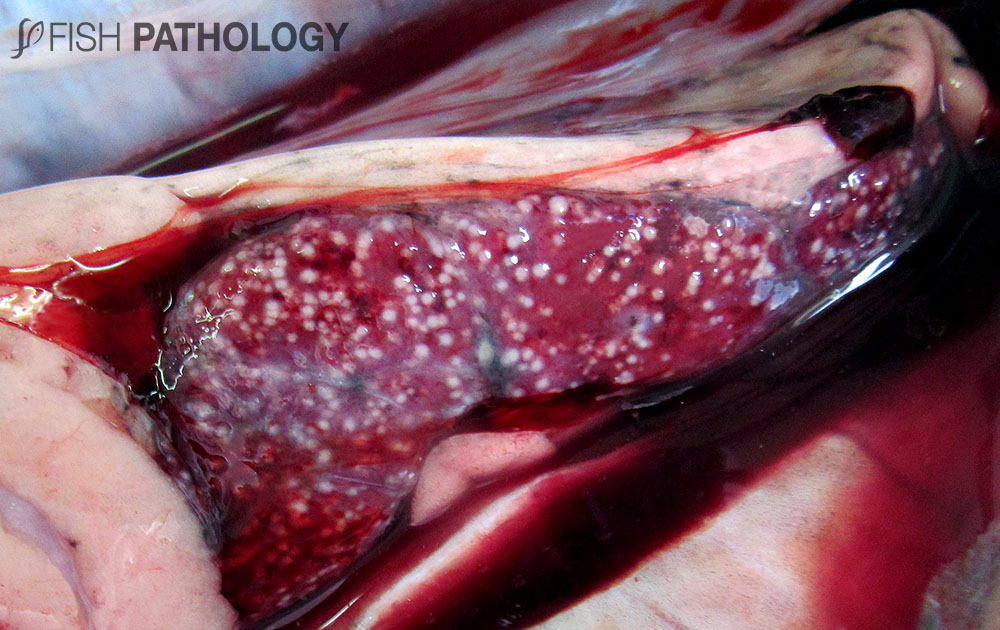
Granulomas are systemic and can be observed in spleen, heart, liver, and of course the kidney from which the disease derives its name. The kidney is generally swollen, and grey-white granulomas of various sizes are seen on the surface of and throughout the organ. Perforation of the overlying renal capsule results in peritonitis, with petechial haemorrhaging of peritoneum and underlying muscle. Peritonitis and/or destruction of sufficient nephrons (impairing fluid balance) can result in an accumulation of peritoneal fluid and a distended abdomen. Peritonitis can lead to the formation of diphtheritic membranes covering all internal organs, most easily seen over the liver and spleen. The heart can be so severely involved as to be almost obliterated, with pericarditis leading to constriction and cardiac tamponade as common sequelae. A yellow, viscous fluid occurs in the intestine and may contain blood.
A seasonal “spawning rash” has been reported in adults around spawning time, where a pustular dermatitis may cover large areas of the skin with many blisters or raised haemorrhagic nodules within the epidermis. Granulomatous tissue invades adjacent scale pockets and extends longitudinally along the fibrous tissue layer of the dermis. These lesions disappear after spawning.